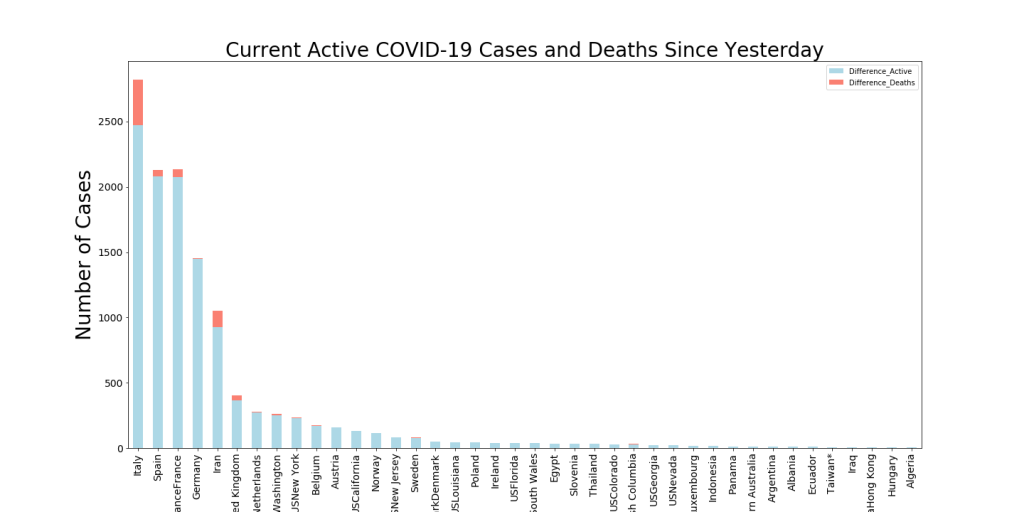
Most European countries are updating their data while we’re sleeping in Arizona. I have re-run analytics and added new ones. Things continue to get worse in Italy, Spain, and Iran. Total numbers of deaths in Italy will catch those in China today or tomorrow and Spain is catching up to Iran. Numbers of new active cases in New York state skyrocketed yesterday. New York and Washington were essentially tied yesterday. Perhaps this reflects that Washington is a week or two ahead of New York and maybe it’s new active cases are slowing down.
World Map showing the areas with the highest numbers of active COVID-19 cases along with the growth in active cases in the last 24 hrs.
US Map showing the areas with the highest numbers of active COVID-19 cases (color – Red is worst) along with the growth in active cases in the last 24 hrs (bubble diameter) .
Since my evenings are less occupied with 7th grade math and social studies homework, I have a bit of time to follow my curiosity about COVID-19 data and trends. I plan to update these daily to provide up-to-the-date visualizations. Here are my starting points… (data from Johns Hopkins Whiting School of Engineering — https://github.com/CSSEGISandData)
This chart shows a couple of interesting things… first, the current state of Active COVID-19 patients (color per the heat map to the right of the image) and second, the number of Active cases that have been declared in the last 24 hours. This gives an idea of both the velocity and the acceleration of the virus in these regions.
For instance, you can see Europe is overwhelmed by new cases (diameter of the bubbles) but Italy has many more Active cases in its medical pipeline than the other countries.
Here’s the daily trend map. Size of the bubbles reflects the New Active Cases in the last day and Color reflects the number of Active Cases
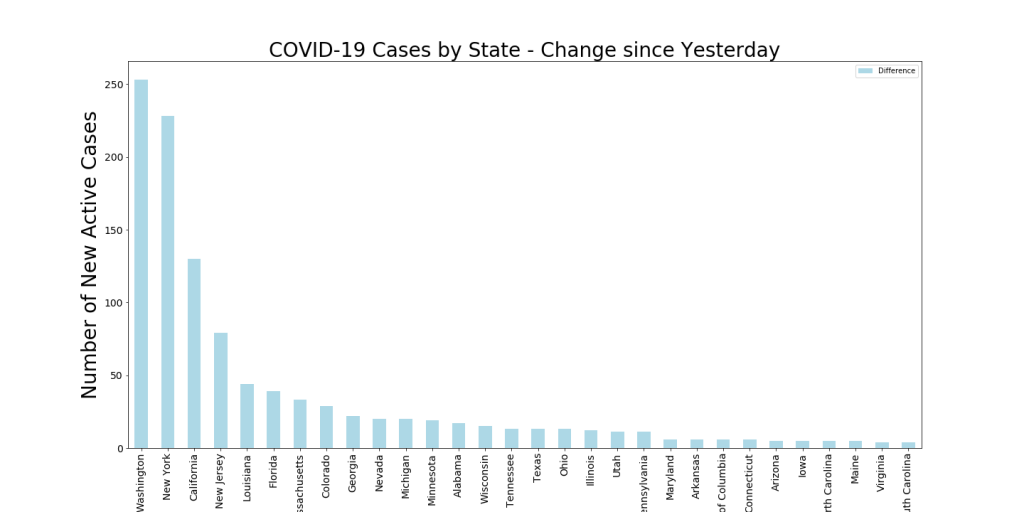
Below is the current change in Active Cases in the last 24 hours by State. Washington has had the most cases (they’re further along) but New York will probably pass them up tomorrow. New York has the greatest total number of Active cases of any state, with just under 1000.
Download a Table of the latest Totals of Active US Cases by State
The Rain predictor has continued working well through the monsoon season. Most predictions have been a couple of hours off, though. During the last week it has predicted four rain events correctly (including the start of our 2019 Monsoon season) and has missed one (see table below in red). The Green or Red labels align with the actual time it rained at the house.
Note this is rain at my house, not just rain in the Tucson area. So that makes it a bit more challenging. For instance, on 7/30, one could see heavy rain all around the Tucson area at the times the model predicted, but it didn’t rain at my house until about 3 hrs after the last predicted time.
Yesterday afternoon at around 4PM (at my house) our first monsoon rainstorm hit with a vengeance! Streets were flooded for a few hours and the temperatures dropped 40 degrees. My rain predictor (see below) predicted this storm 18 hours beforehand, but estimated a time about 2 hrs earlier. This means that the last two times the neural network has predicted rain at my house, it has been right.
See below for latest weekly chart and rain predictions.
Note the humidity spike on the right. Predicting Rain for Monday early AM and slight probabilities again throughout the day. This model predicts rain 12 hours in the future based on the previous 8 hours of data.
Noticed that my rain predictor popped up a strong prediction for about 18 hrs from now. Last time this happened (2 wks ago) it was about 2 hours off on the prediction. Here’s the week’s data plus the prediction chart.
See below for the weeks data and a more believable probability chart. Not sure what happened with yesterdays (It might still rain today as predicted, but I doubt it), but I’m working on it.
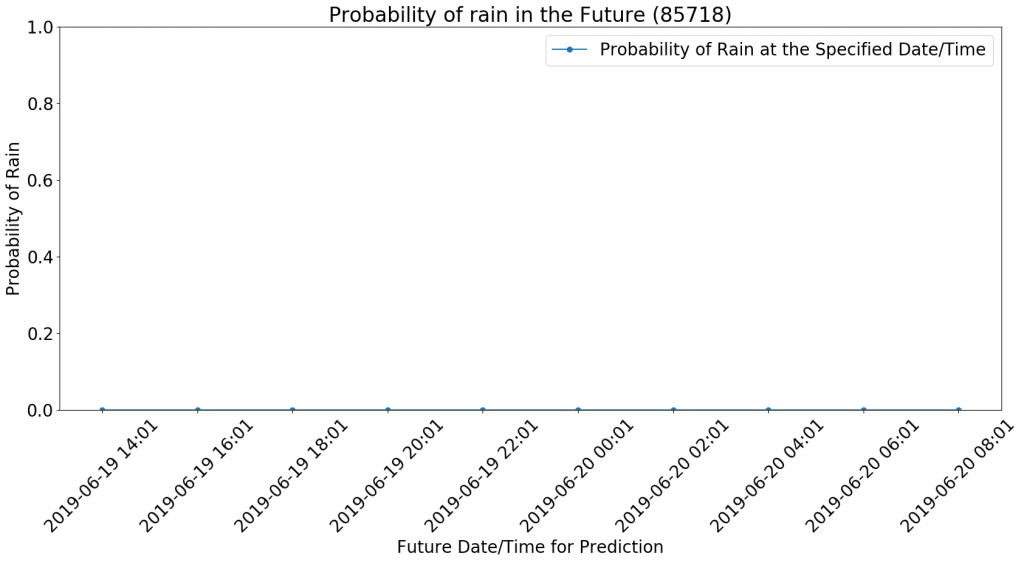
One of my motivators for collecting this data is to figure out how to make predictions using it. I have been running a neural network predictor using this data for a while now with the intent that I could publish rain probability in the future. I have it about ready to show an example. Picking today because the model has made a surprising rain prediction that I don’t understand. (posted on 6/18 at 4PM…)
See graph below to see some of the prediction results. Probability of Rain is predicted for the times referenced.
More on how to design this machine learning workflow.
Tucson has steadied into its early summer weather pattern. You can see this in the monthly plot below. Lower humidity and (of course!) higher temperatures dominate.
Don’t mind the glitch in the middle, my Raspberry Pi is getting tired and sometimes konks out on me when I go on travel!
Over the last 2 days (11/13-14) we had quite a bit of wind in Tucson. These are probably the same winds that plagued California and spread wildfires over the weekend. The winds drove the humidity way down and the temperature followed. Note the large pressure spike (it went just off the scale on Monday). This gradient must have drug the winds along with it, I suppose.
I’m curious about the luminosity spike (both visual and IR) yesterday, because it wasn’t noticeably brighter than the previous few days. Will be watching to see if this is a trend. One hypothesis is that the wind knocked down some leaves from the mulberry tree that protects my porch (and therefore, the weather data collection rig).