Here’s a quick update on what is happening in the US and around the world. See analysis below the images.
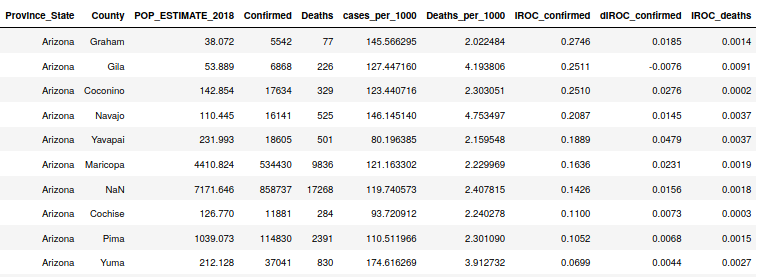
State Data Table, 5/9/2021
A bit over a week ago in my last post, Michigan was leading the US in case rates. Since then, their cases have collapsed and Michigan was replaced at the top by Colorado, then Oregon, then Alabama… This makes me suspect that these outbreaks (they’re all very small compared with the peak in January) are somewhat isolated. Above, the data tells us that the highest acceleration of cases is happening in Alabama but the largest slope (cases per 1000 persons per day) is in Oregon. It’s not surprising to see lots of cases in Oregon as that state has been very lightly touched to date. A similar effect is happening just north of Oregon in Washington. The sixteen states above are the only ones that show a daily increase in the case rate (dIROC_confirmed). The rest of the states are seeing case rates slowing.
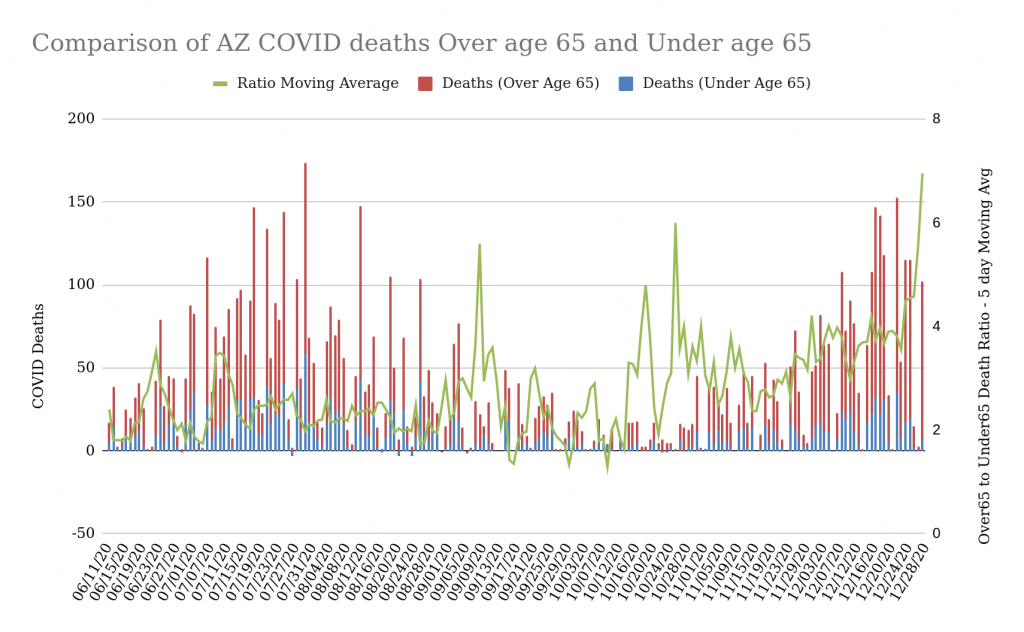
Arizona Deaths due to COVID-19 along with moving average of Ratio – 5/9/21
The above chart shows something interesting that I have highlighted. The Arizona ratio of deaths in the over65 demographic to deaths in all other demographics is slowing significantly. What this might mean:
The data is small (deaths are down significantly) and this is a statistical anomaly.
The over 65 demographic — which seems to be getting close to “fully” vaccinated per the AZ DHS data — is being protected by the vaccine from severe responses to COVID. We all suspect that this is the case, but here’s some data showing a pronounced shift since about mid-March.
World Data
Raw Number of New Active Cases and Deaths on 5/8/21
Above you can see the new cases and deaths on 5/8 from the top 17 countries. There’s lots of news about India and the terrible things happening over there as their hospital system gets stressed, but in actuality, on a per capita basis, India, Brazil, and the US are in much better shape than the leading countries in the chart below. India’s 400K cases yesterday represents about .3 cases per 1000 people, which is about half the number of Peru from 5/8.
Number of new cases and deaths (5/8/21) normalized by population
At some point in early 2021 the more mediocre articles about COVID in the popular media started to slow down and memes in social media began to disappear. Much of the focus in these places turned to vaccines and the new US administration’s approach. It seemed like a good time to slow down my COVID updates and instead spend time watching. For a while I have been concerned that overwhelming people with data and analytics about COVID was contributing to the overall problem of fear and distrust (although it seemed necessary in light of the poor communication from government and media). However, I’ve continued to collect data and run analytics. Here’s the latest data for those who are interested.
Topics:
United States Situation
World Situation
The Latest on Interesting Analytics
United States
Table of US States sorted by Case Slope – 4/27/2021
The above is the table that I have shown throughout the Pandemic. You can scroll back a few pages and see this table during the different outbreaks for comparison sake. Right now there is one big outlier, Michigan, interestingly one of the states with the most restrictive (or at least publicized) COVID policies. The good news is that Michigan’s current case rate is still only about half of what the highest state was during the winter outbreak. The next highest regions have significantly lower slopes. This is an unusual trend and may be indicative of the success of the vaccination policies that the states have put in place.
Table of Counties in Arizona sorted by Case Slope – 4/27/2021
Arizona has significantly lower Case Growth than other states right now. The highest counties in the state are those who were spared a bit more during the recent outbreak. This has been a pattern throughout… the virus finds regions that haven’t been hard hit and then runs for a while until it runs out of targets or temperatures move outside the virus’ comfort zone.
One metric that I have been tracking is the ratio of deaths in groups over age 65 to deaths in groups younger than 65. In Arizona, only around 13% of the population is over 65 but this ratio is still somewhere about 3:1. This is a sign of how overwhelmingly COVID has impacted the over 65 age group. During the first large summer outbreak in AZ we saw a ratio of about 2.3:1. During the most recent winter outbreak, we saw the ratio peak up over 3. This increase might mean that right now there are less susceptible people under 65 than there was during the summer of 2020. The green line on the chart above is the moving average of this ratio. The recent peaks in this line are primarily due to the small numbers of deaths being recorded now.
Here we see the case growth curves for both Maricopa and Pima counties with the number of COVID tests per day superimposed. This metric (number of tests) is not a perfect metric but it appears to be a solid indicator of upcoming acceleration or deceleration in the COVID case curve. You can see for yourself that when it starts trending in a direction, a change in the case curves comes 4-5 weeks later. Currently the number of tests is approaching the low water mark but this remains a good number to keep watching to give us an idea of whether there will be summer outbreaks again this year.
Arizona %Tests Positive by Day – 4/27/2021
This chart shows the percent of tests conducted yesterday with positive test results. The blue dots are the daily results and the gray curve is the best-fit line that describes the trend. The tests positive number hovered near 50% for a while and now is stable around 8-10%. It is concerning to observe that the curve shows signs of turning up again. If true, this may be an indicator of another summer outbreak in Arizona.
World Data
Table – COVID Data from Around the World, Sorted by Number of New Cases – 4/27/2021
India has been in the news recently for their large number of new cases and deaths. 323K new cases in a day would be enough to intimidate anyone. The raw numbers seem scary, but note that the case slope (IROC_c_n) is very low for India (.2724). What this means is that right now, as a percentage of their population, the rate of new cases is quite a bit lower than other countries (see below). If one considers case acceleration (dIROC_c_n), we still see that India’s number of an increase in .008 cases per 1000 persons every day is small compared to countries like Turkey, Columbia, and Argentina.
Table – COVID Data from Around the World, Sorted by Case Slope – 4/27/2021
We can see that India isn’t even in the top 10 in the world with regard to normalized case slope (IROC_c_n). Turkey, however, is very interesting with both a high raw count of cases and deaths, but also a very high normalized Case Slope. Turkey also has a very large population, but not nearly as many as India, so their numbers of new cases each day will be shocking (43K yesterday), but not as difficult to comprehend as the 323K new cases yesterday in India. So even though India isn’t as fully-saturated with COVID as Turkey or some of the South American countries, it’s still a problem for the world. India is one of the largest manufacturers (maybe the largest) of pharmaceuticals in the world. COVID vaccine manufacturing has dropped significantly since the start of India’s second wave. This is an example of how COVID can drive non-linear effects.
Updates on Interesting Analytics
Normalized Cases and Deaths by Latitude Range – 4/27/2021
I have showed the above a number of times during the pandemic. The trend still holds where the latitudes between -10 and 20 have experienced very few cases and deaths due to COVID.
Factors correlated with Cases per 1000 persons – 4/27/2021
I have also shown multiple revisions of my correlation studies over the last year. In the above we are demonstrating the levels of correlations of various measurable features with cases per 1000 for countries across the world. The top factors associated with COVID cases continue to be smoking and BMI metrics. What this says is that in regions where smoking rates and Body-Mass Indicies are high, we have seen larger numbers of COVID cases. It may not be surprising to see this. Population over 65 is also another feature highly correlated with Cases per 1000 and the inverse correlation of COVID cases with the prevalence of Tuberculosis in a country is still quite interesting. I know there were some studies into whether TB innoculations were somehow providing protection against COVID, but I lost track of those.
Factors Correlated with Deaths per 1000 persons – 4/27/2021
The above correlation is for death counts per 1000 persons. As with the Case correlation project, we see that smoking and BMI measures are strongly correlated with COVID deaths. Population size over age 65 is also (unsurprisingly) correlated with COVID deaths as well. For some reason, the growth rate of the country is inversely correlated with COVID deaths. Perhaps this is because a region that is growing is adding infrastructure like hospitals? This might seem to contradict the observation above that the number of hospital beds is correlated with COVID deaths, but my suspicion all along has been that countries with large hospital bed counts are probably recording more COVID deaths that go unrecorded elsewhere.
It’s pretty interesting to see that the COVID case/death trends by latitude have continued. I suspect some of this could be attributed to a lower population in some latitude bands combined with a focused COVID outbreak, but since this is population-normalized, it probably only applies at the 50 degrees and northwards latitudes…
Equatorial regions still have a significantly lower case and death count. Poorer reporting could be partially involved, but can’t describe this big of a difference. Surprised this isn’t discussed more.
COVID-19 Cases/Deaths per 1000 persons by Latitude – 2/11/2
Around the end of January I posted this table and about half or less of the states were showing deceleration of their COVID case growth rates. This could be seen in the dIROC_confirmed column where negative numbers are deceleration and positive numbers are acceleration. Now, about 12 days later, every state has negative growth acceleration and the overall growth rate numbers are much lower. This happened very quickly. You can see that Arizona — who had the largest growth rate in the country as of 1/31 — now is much lower and has the largest deceleration number in the US.
As winter weather patterns still differ across the US, I’m curious if this reflects growing numbers of COVID vaccinations
COVID-19 Data by State – 2/11/21
Below are the Arizona numbers by county. One interesting point to note is that Maricopa County has a higher deceleration number and a lower overall case growth rate than Pima County. This is counter-intuitive because Pima County has enforced much more restrictive COVID policies during the entire outbreak. I have heard (but haven’t researched) that vaccines are easier to get in Maricopa County due to a more efficient rollout by their County Medical Office. Perhaps this is reflected in these numbers?
Here’s the current state of the primary analytics that I maintain on a daily basis. The data for these comes from the Johns Hopkins University and from the AZ DHS. Occasionally the data diverges between these two organizations, but not wildly.
I thought it might be interesting to share what I look for in these tables and graphs, especially now that the case rates are slowing down in Arizona and across much of the US.
COVID-19 Basic Data Table sorted by Case Growth Rate – 1/30/21
The above table is familiar to anyone who has read one or two of these pages. It sorts each state by their overall case growth rate. I call this the Instantaneous Rate of Change (IROC) because what I’m measuring is the current slope of the COVID Case curve. The states can be compared because the COVID cases are normalized by each state’s population. This table can help one to quickly identify where the hotspots in the US are. The Confirmed Case IROC tells us how many Cases per 1000 persons per day each state is experiencing. I sometimes refer to this as the case growth rate. The dIROC_Confirmed column tells us how fast the case growth rate itself is increasing. Above, we see that Arizona has the largest case growth rate in the country but that this growth rate is decreasing by 0.0275 cases per 1000 per day — every day. When a state’s dIROC_Confirmed starts slowing, it is an indicator that the case growth rate peak is near. When the dIROC_Confirmed goes negative, it is a sign that the peak is in the past and the case growth rate is now decreasing. I captured this table all the way down to California, who about 2 weeks ago had the highest case growth rate in the country by a pretty good margin. As you can see their case growth rate continues to decrease every day. It looks like Arizona will be seeing similar numbers in about a week since it’s peak was about a week and a half ago.
This table also tells us interesting things about cumulative numbers. You can see that Arizona, Rhode Island, and Utah all have very high cumulative cases per 1000 population. This probably reflects the overall populations of these states being smaller or more confined to larger population areas. Much of Rhode Island’s population is near Providence, Utah’s population is primarily in the Salt Lake area, and a majority of Arizona’s population is in two metro areas, Phoenix and Tucson. Also, most of these regions have seen recent case surges while states like NY, MA, and NJ have had a long lull since their primary surge back in March. One other metric on this chart that’s useful to understand the state’s situation is Deaths per 1000. The Northeastern states still have the largest number of deaths per 1000 persons, but other states like Louisiana, Mississippi, and Arizona are catching up.
Arizona Case, Death, and Hospitalization Data
Arizona Cumulative Case Curves by Age Demographic (cases per 1000 person in age group) – 1/30/21
Now I’m switching primarily to Arizona numbers. These may or may not be similar to what is seen in other states, but I have pretty good access to Arizona data as well as the motivation (being an Arizona resident) to tracking them more closely.
The above chart is the visualization of the Case per 1000 curves for five different age demographics in Arizona. During the initial summer case surge, it was clear that all the age groups between 20 and 54 tracked together and had the same case rates when normalized by their population numbers in the state. The 65+ group has tended to have lower cases per 1000 and the under 20 group has far lower cases per 1000. This chart tells us that this trend continued until about mid-November, when the 55-64 group really separated from the herd (this is the green line above). It also appears to the naked eye that the 65+ line (maroon) also had a slightly increased slope over the under 55 groups starting around mid-November. As I’ve mentioned in other postings, this likely represents contribution to cases from winter visitors to Arizona, none of whom are represented in the Arizona population for their age group. Therefore, they’re contributing to the numerator (cases) without contributing to the denominator. This may just be a curiosity, or maybe it has a hand in Arizona’s particular COVID case and hospitalization challenges since the beginning of October. It appears to me too that while the age groups under 54 (red, yellow, and blue) have started significantly flattening out — meaning that their growth rates are slowing) — the over 55 groups seem to be slowing less.
Maricopa and Pima County (AZ) Case Growth overlaid by Statewide Tests per Day (5 day moving avg) – 1/30/21
The above is a chart that I look at a lot and like because it compares the case curves for Maricopa County (Phoenix) and Pima County (Tucson). This is interesting as a natural experiment, because it seems provable that Pima County has imposed much more structure around COVID protocols than Maricopa County and has done so pretty consistently since the beginning. The Blue line is the polynomial equation fit to the Maricopa actual case data (light grey) and the Red line is the equation for Pima actual data (dark grey). The change in the current surge rates is revealed where the real data diverges from the polynomial. This started around the first week of January, but I could see signs of it beginning at the start of 2021. The other interesting signal in this chart is the moving average of tests per day in the state. I’m only showing the numbers of tests, not the positivity of these tests, in this chart because my theory is that the number of tests is a leading indicator for case growth (this likely measures how sick people think they are… few people get COVID tests for fun, I’ve observed). Looking above, you can see that the number of tests moving average hit a low around 9/08 when the case rates were increasing only a slight amount and appeared to be doing so linearly. The case rates started curving upward somewhere starting early October and the test numbers increased along with it. The test number peaked somewhere around the holidays and then gradually slowed. This may have anticipated the case rates starting to slow somewhere in early 2021. This may or may not really be a leading indicator, but the data I have makes it seem interesting at least.
Comparing Deaths over 65 with under 65
Arizona deaths – Over 65 age group compared to all age groups under age 65. Overlaid with the moving average of the 0ver65 to Under65 death ratio. – 1/30/21
The over 65 population in Arizona makes up about 13% of everyone in the state, but has experienced most of the deaths. At some point, I started tracking the Over65 to Under65 ratio as an indicator. You can see the above as the green line. This is the 5 day moving average of this ratio. The light blue bars are raw deaths for the under 65 group (87% of the population) and the red is the raw deaths for the over65 group. The right way to show this data would be normalizing it by each group’s population, but if I did that, the blue wouldn’t be visible unless I plotted it on a logarithmic scale (very hard to explain to non-math majors). The green line is maybe the most interesting element of this because of the comparison of the ratio during the smaller summer outbreak (June/July) where the ratio hovered around 2.5 with the ratio during the current surge, where the ratio jumped quickly and has been ranging between 3.0 and 4.0. This is hard to analyze, but it appears like the virus is more deadly now for the older demographics than it was during the summer. Perhaps the cooler weather compounds the virus’ effect or perhaps there are less susceptible persons under 65 now than there were during the summer? If you’re curious about the spikiness of the ratio during the lull from August until October, I’m pretty sure it’s just due to the small numbers of deaths during that time frame. Small data’s statistics can behave oddly.
Hospitalization Analytics
Percent of Cases (by age group) hospitalized one week later – 1/30/21
Above is what I call my “experimental” metric on a ratio of current hospitalizations to cases from one week earlier. As you can see above, I do this ratio for each age demographic. The basis for this analytic is that I was curious about the rate that people get hospitalized one week after they are confirmed with COVID. Perhaps 2 weeks might have been a better gap, but I chose to use one week because I felt that might be a more common time frame between a case and a hospital visit (any kind, ER, ICU, Outpatient, etc.). Each datapoint represents the daily ratio and since the trends are hard to see with the naked eye, I fit a regression line to each age group so I could see the trends. It doesn’t show it here, but though all the trendlines on this ratio show a decreas now, but back around November, the over 65 group’s trendline was increasing pretty steeply. This changed sometime around the holidays and all the age groups have been trending down ever since. This indicates to me (but doesn’t prove, of course) that hospitalization surged in the over65 group pretty strongly early in this outbreak. It was likely this over65 group that filled the hospitals (see below) very rapidly starting November 1. You can see above that the maroon and green (over 65 and 55-64) dots around that timeframe frequently ranged between 50 and 75%. This means that the number of people hospitalized during that timeframe over 55 was 50-75% of the Confirmed Case counts for those demographics one week earlier. Now the numbers for over65 are generally under 25% and the 55-64 are generally under 10%. This is not a perfect metric, but it does seem to be illustrating a trend and was possibly a good leading indicator for the COVID hospitalization easing that can be seen below.
ICU Bed Chart from AZ DHS Dashboard (compares COVID beds to non-COVID and Available Beds. 1/30/21
Finally, I’ll re-show the latest from the AZ DHS on the breakdown of COVID, non-COVID, and empty ICU beds in the state. This is a stacked bar chart and the three states above add up to 100%. So for instance, at the hospitalization peak around Jan 5th we could see just over 60% of the ICU beds in the state occupied by a COVID patient, about 30% of the ICU beds occupied by a non-COVID patient, and about 10% of the ICU beds empty (my guess is that these were the broken ones??). Today, we see about 50% COVID, 40% non-COVID, and still 10% unoccupied. If this follows the trend from the summer, we’ll soon see the COVID hospitalization numbers start dropping even faster.
The Case data for the Arizona winter outbreak has shown some unusual characteristics that might be unique to the state. The chart below shows a few of these anomalies.
The cases began acceleration almost to the day that temperatures in Phoenix dropped from 15 to 20 degrees F overnight. The cooling trend only stayed for a few days (see the orange and blue bar chart below), but nighttime lows remained lower until November 8th when the temperatures plummeted about 20 degrees again. These drops plus the movement of the nighttime lows below 60 degrees seems to have triggered the case acceleration that has only recently began to slow.
The green line in the diagram below represents the 55-64 group. This plus the 65+ group makes up the bulk of Arizona’s annual winter visitor population. Arizona State University did a study a few years back that showed that the population in the Phoenix metro area swelled by 300,000 every winter. I have heard that Tucson’s population increases by over 100,000 every winter and areas in the western part of the state (such as Quartzite) are said to have over 2M visitors every winter. So why is the 55+ groups both accelerating faster than the 20-54 groups? My guess is that the winter visitors are bringing COVID cases with them, and since I’m normalizing by the population of these age groups that lives year round in Arizona, I’m showing a higher number of cases per 1000 “year round” residents. I suspect if I could correct the denominator of this ratio with the actual numbers of full-time plus winter residents each month, then the rates would equal the 20-54 groups. What does this tell us? Some decent percentage of our case counts during the winter outbreak are due to winter visitors. (edit: Using some back of the envelope math I arrived at about 10K cases in the 55 to 64 age group due to winter visitors. This would mean there have been around 90K winter visitors in this age group since November)
Just before Thanksgiving the case rate appears to have slowed a slight bit, but around the end of November, we start seeing strange case count disruptions and apparent acceleration. Looking closely (I’ve blown this range up in the graphic right after the one below), it seems like a short glitch that is probably due to cases being counted inconsistently during the holiday break. Some days had no cases reported and others had nearly as many positive cases as tests. Obviously that was the state catching up on counts they had accumulated when they were out of the office. I don’t see any strong evidence of a holiday surge for either Thanksgiving or Christmas. At best there could have been a slight acceleration, but it appears more likely that inconsistent data collection may have given the impression of a short uptick in cases.
The under 20 age group (blue curve) continues to show that the rate of infection in this group is significantly lower than the other groups. This may be due to our inability to measure these cases well (since so many are asymptomatic) or due to this group’s lower probability of getting infected. Or maybe it’s because this group is more sheltered than others because they stay at home, don’t need to go to work, aren’t buying groceries, etc. Or some combination of these. Remember from my recent excess death analysis that this age group had around 1/2 (on average) the deaths during 2020 than would be expected in a normal year.
For the last week or two, the cumulative curves for all the groups (less so the 55-64 group) show obvious deceleration. This coincides with the decrease in COVID hospitalization that I show below.
Arizona Cumulative Case Curves (per 1000) by age Demographic – 1/20/21
Below you can see the zoomed in area where the data glitches occurred. The overall case slope during these times appears to be constant, so the appearance of case acceleration during the holidays is probably due less to a holiday surge than to poor data collection.
Zoomed Range from the Above Chart – 11/15/2020 to 1/20/202
Below is the hospitalization chart from the AZ DHS dashboard. It is a stacked bar chart, and the combination of the colored bar percentages will add up to 100%. The Red bars reflect COVID cases in the ICU (60% of all ICU beds today) whereas the dark grey reflect non-COVID ICU beds (about 30% of all ICU beds today). The light grey is the unoccupied beds (about 10%). As you can see the numbers of beds occupied by COVID patients has consistently been dropping for a week or two. This is consistent with how the Summer outbreak worked. Hopefully this means the hospitals are through the worst of it.
Here’s a map of the top 200 AZ zip codes by COVID case growth between 12/21 and 1/13.
Note that the dark blue dots are around 20% growth over these 3 weeks and the orange and red dots are around 80% and 90% growth. That’s a pretty big range.
The zip codes with higher percent growth look to be on the fringes of the more dense, inner city zip codes. See how the Dark Blue seems to be ringed by lighter greens and yellows in the Phoenix area. This may be a factor of how this is measuring growth as a percentage of what it was 3 weeks ago as opposed to raw case increases. Might be interesting to think about.
Lots of zip codes in small towns in rural counties with large percent increases in cases.
Map of top 200 AZ zip codes by case growth from 12/21 to 1/13
This is a follow-on to two previous analyses (here and here) of excess deaths during 2020. My approach is different than most (or all) I have seen because I am looking at the impact of COVID through evaluating excess deaths in all 10-year age demographics across all US states and DC. What this does is set all demographics equal regardless of their population. I think this is a very reasonable approach because I’m primarily focused on learning what the impact was to each demographic through measuring the percentage of excess deaths (over an average from the two previous years with good data, 2017-2018) while also maintaining awareness of that demographic’s COVID impact. Note that this approach provides some interesting insight.
Caveats
As I don’t want people to think that this work is conspiracy-based or whatnot, I want to make my assumptions clear here. First of all, I assume the Provisional COVID and total death data for 2020 from the CDC is correct. Or at least that it is not wildly incorrect. The CDC has made some mistakes and their analysis of their own data is often suspect, but it does seem like they’re being very careful not to mess up COVID data. Second, I want to reiterate that my approach is different from most you may have seen. This excess deaths analytic gives equal weight to every state and every 10-year demographic. Therefore, 1-4 year olds in Rhode Island have as much impact in the histogram below as 85+ year olds in New York who had very high numbers of deaths due to COVID. I think this is interesting, because COVID has impacted all of society differently. For some it has been devastating in loss of life but for others it may have been devastating for other reasons. Most analyses of excess deaths by the CDC or popular media is only focusing on the raw deaths, which overwhelmingly have come from the oldest demographics. Third, I am only using a two year set (2017 and 2018) as a baseline for the excess deaths. I could have used a 5 year average, but I chose to use the two most recent years with good death numbers to minimize the impact of growing US populations (because larger populations experience more deaths). It turns out that one of these years was a bad flu year and the other was an easy flu year, so that is serendipitous too. Data from the CDC on provisional deaths for 2020 can be found at this URL and the 2017-18 data can be easily captured on the CDC’s “Wonder” system
Histogram of Excess Deaths by Demographic and State
Histogram of excess deaths for all demographic/state combinations
Takeaway from the Histogram
This doesn’t tell us that we didn’t have excess deaths overall in 2020, so don’t be tricked. What this does tell us, however, is that the majority of state/demographic pairs didn’t have any excess deaths during 2020 over the 2017-18 average. You can also see that the numbers of demographics that experienced more than 100% excess deaths drops off very rapidly (probably at an exponential – e^n – rate) while the under 100% excess death demographics ramp up to the peak at more of a polynomial (maybe n^2 or n^3) rate. This tells us that the demographics across all states were more likely to experience less than 100% excess deaths during 2020. We’ll look at the data tables below to try to figure out both sides of the peak on our histogram.
Data Table – Highest Excess Deaths
Comparison of CDC 2020 Provisional Deaths with Average from 2017 and 2018 – sorted descending by Excess Deaths
Takeaway on Demographics with High Excess Deaths in 2020
The first thing that stands out in the above table is the large number of demographics in DC that are at the top of the excess death list. I have no idea what happened in DC this year to contribute to all these excess deaths, but only a couple of the demographics have large COVID impacts. (Edit. It struck me the reason is most likely because including DC in this analysis is like comparing deaths in Chicago with those across the whole state of Illinois. DC is more like a large city and therefore has unique death statistics)
Secondly, I also notice that there is a mix of “high-COVID” demographics and “low-COVID” demographics at the top of the table. I think most people would have expected the demographics with the most excess deaths to be over 65, but that isn’t the case. Of course, this is on a percentage basis. The demographics with the highest raw number of deaths are mostly over 65, but these are all demographics that experience higher numbers of deaths overall every year anyway. This is why I look at the percentages. Below are the demographics/states with the highest number of raw excess deaths (column on the right). Nothing much is surprising here. Elderly demographics in large states would be expected to have the most raw excess deaths because they have the highest number of deaths every year. This is a good way to parse the data if one is in search for nerve-wracking numbers, but it doesn’t give us any information we couldn’t infer on our own. It is clear, however, that in these groupings COVID deaths were significant, running from 15 to 31%.
Data sorted by “raw” excess deaths in 2020
Secondly, I also notice that there is a mix of “high-COVID” demographics and “low-COVID” demographics at the top of the table (the one sorted by percent – two above). I think most people would have expected the demographics with the most excess deaths to be over 65, but that isn’t the case. Of course, this is on a percentage basis. The demographics with the highest raw number of deaths are mostly over 65, but these are all demographics that experience higher numbers of deaths overall every year anyway. This is why I look at the percentages.
In the next table, I’ll rank the demographics by excess deaths after COVID is subtracted out and we’ll see some interesting results.
Data Table – Sorted by Highest Excess Deaths if COVID/Flu/Pneumonia numbers removed
Data Table sorted by excess deaths after COVID/Flu/Pnemonia removed
Takeaway on Groups with Excess Deaths beyond COVID
The thing that will probably stand out in the above table is that only two over 55 demographics exist in the top excess deaths once COVID and related illnesses are removed. Both are in Washington DC (again, I need to figure out why DC has so many excess deaths across the board. Are they counting differently?). All of the groups above still have excess deaths beyond the 2017-18 average even after the COVID numbers are subtracted. What might this be counting? Arizona, Tennessee, and Colorado demographics under age 44 are all over the top of the list. We know that these states tend to have above average suicides each year. I have also seen reports that deaths due to drug overdoses are exceptionally high in 2020 in younger demographics. This is kind of hard to think about, but it would seem that these excess deaths in 2020 by such large numbers are correlated with COVID and state reactions to COVID.
Data Table – Ratio of Highest COVID+Flu+Pneumonia 2020 Deaths to 2017-18 Average Deaths
2020 to 2017-18 Average Death comparison – Sorted by Ratio of COVID+Flu+Pneumonia to 2017-18 Average
Takeaway on Demographics with High COVID/Flu/Pneumonia Impact in 2020
Note that the above table is as expected. The highest percent impact of COVID/Flu/Pneumonia are in the over 65 year communities. The numbers are pretty staggering though. In the typical year, 30% of a community’s deaths are due to heart disease and about the same percentage to Cancer. The other 40% of deaths are a mix of everything from respiratory diseases to accidents to suicide and homicide. So for a demographic to be seeing 20 to 30% of its deaths in one year to COVID is incredibly catastrophic. I also notice that the Dakotas are very high on the list for their over 65 demographics and wonder if they saw much higher excess deaths due to a lack of government COVID controls (they both seem to have been known for a more Sweden-like approach). I also see a couple of under 65 demographics on this list, both from New Jersey. That would be an interesting thing to analyze.
Data Table – Sorted by Lowest Excess Deaths over 2017-18 average
Data Table sorted ascending by Excess Deaths
Takeaway on Demographics with Low 2020 Excess Deaths
The above is a very interesting way of looking at the data. What does it tell us? 2020 was a very safe year to be under 14. Why was this? I’m not sure, but I’d guess that many causes of deaths for these groups were avoided this year due to locking down at home. Car accident deaths, other accidents, possibly flu and other viral diseases, etc., might have been in very short supply for these younger groups. Interestingly, New York State has two older demographics in this list. If one looks deeper at this, one finds that New York has really low numbers of excess deaths in general. The chart below shows the raw numbers of excess deaths for the over 85 age demographic across all 50 states. You’ll notice that NY actually experienced LESS deaths in this demographic than expected. Perhaps this has to do with the lower mobility of this group during COVID (a good number are likely in nursing facilities where they can’t come and go or receive visitors).
Excess deaths by raw count in over 85 demographic
One big takeaway, however, is that if one was to evaluate the “silver lining” of 2020 by measuring Years of Life Lost, the low incidence of deaths in the younger groups would certainly carry a lot of weight.
Conclusions
COVID does not seem to be the overwhelming contributor to excess deaths across all demographics in 2020. This does not seem intuitive, but the data (assuming it is accurate) does make a strong case that the most impact of excess deaths in 2020 went to demographics who had lower incidence of COVID-19. This is calculated on a percentage of excess death basis, not raw numbers. Perhaps this is the right way to look at the excess deaths though, as compared to raw counts. It does capture surprise and impact to the affected group to look at the percentage of change. Plus, if one simply subtracts the COVID percentage from the Excess Death percentage, many of the younger demographics high on the list would still have well over 110% excess deaths. The older demographics do not see this same effect. What does this mean? Some demographics (younger adults and older teens) experienced significant excess deaths due to something other than COVID in 2020.
COVID did have a terrible impact to a large number of the older demographics across many states. Some of these demographics saw numbers of COVID (and pneumonia and flu because they’re hard to separate out) in 2020 that ran between 20 to 30 percent of the 2017-18 average. This is in the range of heart disease and cancer, each of which contribute to 20-30% of all deaths in a normal year. These groups made up the overwhelming majority of deaths in all regions during 2020.
For Americans under 14, however, 2020 was a very safe year. Much safer than the 2017-18 average. It appears that though the COVID responses may have had an adverse impact on some demographics, it had a very good impact on the folks under 14.
I thought folks might find it interesting to see the cumulative case rate charts from a selection of states and counties. There are interesting things to note in all of these. Remember that these are all just measuring cases and that cases are a strange measure due to the wildly different response different people have to the COVID-19 virus. Still, case growth is a leading indicator for hospital overload and deaths…
Note: in all of these charts, I am choosing to show “non-normalized” data. This means, when you see an “IROC-Confirmed-Case” number, that refers to the instantaneous slope of the curve. This slope will represent the number of new cases per day for the curve, and is often a better indicator of the case growth than moving averages or other such approach. Therefore, when comparing charts, keep in mind that the visual slope of the line is the better comparison than the numbers (because larger places like LA county will most likely have more cases due to their population). Also, I start each chart at the point they hit 5000 cases.
Also, the light blue line might be confusing to people. I am modeling the entire outbreak in a region with a fourth-order (quartic) polynomial equation and this equation is plotted in blue. You can see how the red “actual” datapoints often align strongly with the quartic equation for the region. I’m not sure if the fact that I can fit the whole outbreak for a region with a quartic is interesting or not, but I do know that the quartic emerges often in fields like optics and the propagation of waves through a real-life transmission line (like a copper wire). I wonder if a virus propagating through a real society is a similar application?
Pima County, Arizona, 1/4/20
I’ll lead off with the chart of my home county. Pima is the location of Tucson and has over 1M in population. Mask orders have been in place since early June, but my observation was that a lot of residents were already observing mask orders well before that. The whole county has a curfew currently in place (I assume it is to reduce the numbers of people at bars?). You might note that the curve was solidly accelerating from about Halloween until Thanksgiving and then it started into a linear phase comprised of a bunch of positive and negative oscillations. This is to say, that the case rates have slowed for a few days, then sped up, and so on. Note that the last data point is a big jump over previous days. My guess is that this is an anomaly due to state DHS people taking holidays and accumulating numbers differently than in the past. Today’s data point (not shown here yet) is much lower, so I’m curious about whether the deceleration trend continues or not.
Maricopa County, Arizona, 1/4/20
Maricopa county is the largest in the state with over 4M residents. This is the location of Phoenix, Mesa, Tempe, etc. Note that the latter part of the chart looks similar to that of Pima County. You can see more of the Maricopa curve since they hit 5000 cases earlier than Pima. Right now Maricopa communities have individual mask ordinances in place (some cities cancelled theirs then brought them back as cases surged. I’m unaware of any curfews in Maricopa, but that may be from lack of looking. Maricopa County is also the location of a number of large kids soccer tournaments back in late November and early December that were notable due to media attention (lots of teams from California were participating since they can’t practice or play in California). I don’t see any evidence of case surges due to these tournaments… rather, it appears like cases decelerated all the way from Thanksgiving until about Christmas day.
Los Angeles County, CA, 1/4/20
Currently, California has the highest case acceleration of any state and it does seem like LA county is a big driver. Note that the curved formed by the red datapoints is steeper than the blue line would model. This is very surprising to me in light of California’s significant COVID-19 restrictions. One might speculate that high density plus low evening temperatures (in my previous entry or two I point out that most of these surges started when night temperatures fell to 50 degrees) could be leading to the really steep slope in California. However, density might not explain it, as I’ve noted in Arizona that the most dense zip codes tend to have lower case growth than the less-dense zip codes. Regardless, the situation in CA is a puzzle.
Orange County, CA, 1/4/20
Orange County’s case curve looks similar to LA’s except it seems to fit the quartic model better regarding acceleration.
Harris County, TX, 1/4/20
Now we’ll switch to another large county, Harris County in Texas. This is the location of Houston. Note that it’s case slope is much flatter than any of the other regions. It appears to be accelerating slightly. One thing I’d note about Harris County that is absent in the previous charts, and that is humidity. Whereas Arizona and California are very low in humidity this time of the year, Houston is somewhere around 70-80% humidity. It has been observed that the virus transmits most effectively in lower temperatures and low humidity.
New York State, 1/4/20
Above is the chart for the state of New York. It looks similar to California, just with a bit lower slope. The state also seems to have the same oscillation pattern over the last two weeks that AZ and CA regions have.
Pinal County, AZ, 1/4/20
Now to change the pace again, here’s the third largest county in the state of AZ, Pinal County. This is a mix of rural and suburban communities, probably leaning more towards the rural. To my knowledge they don’t have any county mandates in place for COVID-19 and their characterization through 2020 regarding COVID leaned more to the individualistic rather than the collectivist. Pinal saw some notable tapering off of the visual slope of cases around 12/15, but some of this is probably anomalous due to the large jump that happened around 12/13. This has the appearance of being a data collection glitch. Note though, that this county’s trend is to fall below the blue quartic model line.
Finally, here’s a picture of a much smaller county in AZ, Cochise County. This is a primarily rural county with a medium-sized retiree population. Cochise had very few cases for the longest time but they’re getting close to doubling their case number since mid December. This is another area that has hit lows of 50 degrees and has low humidity. It is a bit higher in altitude than Pima County.
Normalized Data for Selected States
Cases per 1000 persons, selected states, 1/4/20
Here’s a chart where I have normalized the data by population to give better comparisons. I’ve selected a handful of states, including a number from the section above. What do we see across the board? General slowing of cases across the southeast, a bit of acceleration remaining in California and New York, and a bit of “uncertainty” in places like Georgia and Arizona.
The diagram below shows COVID rates per 1000 person of the affected age group. So for example, currently the 55-64 year grouping has seen close to 100 members out of the total Arizona 55-64 population come down with COVID-19. This helps us understand how each age group is affected by COVID. We know that there are far more 20-44 year olds than any of the other groups, so obviously they have more COVID cases. But when you divide by the total number of 20-44 year-olds in AZ do they see a greater rate of infection? As you can see below, no, they’re near the top, but they’re actually below the 55-64 group and right equal with the 45-54 group. This is pretty interesting and gives us some food for thought:
The 20-44 and 45-54 groups make up the majority of the active workforce and are more likely to be taking public transportation to work.
These two groups are also probably more likely to be working out in gyms and going to bars.
From my observation (no data to prove this) all the groups other than the less than 20 appear equally likely to be going to restaurants.
Why has the 55-64 group accelerated ahead of the other groups though? You can see they were right there with the 20-44 and 45-54 groups right around mid-November. One guess that I might hazard is that this is a reflection of growing numbers of 55-64 aged persons in the state from winter tourism. This would cause the number of persons in this group in the state to increase from the standard number of permanent residents that I use for the rest of the year. Note that the slope of the 65+ group also seems similar since Mid-November to the 55-64 group, but the slope of the 20-54 grouping (most likely there are few winter visitors in this group) is lower. So I suspect we’re seeing an increased COVID rate in AZ since mid-November due to an influx of winter visitors.
Note that the 20-44 and 45-54 groups have the appearance of a decreasing slope and the under 20 group definitely has the appearance of a decreasing slope. This makes me think that the disease is slowing in its transmissability and we will continue to see case rates flatten out in the next week or two. Other reasons I might think this is because hospitalization rates have been slowing for a week and a half and death rates in the under 65 groups have also slowed significantly.
The below is the hospital bed comparison from the AZ DHS COVID dashboard. The red bars represent the % of ICU beds (in this case) that are in use by COVID patients. The dark grey is all other patients and the light grey is available beds. Note how the red bars are starting to trend over. This is a sign that the hospital COVID recoveries (and deaths, I suspect) are starting to exceed new admissions. This could be a false alarm and the hospitalizations will spike, but it doesn’t seem to be the way this disease works. Note that there are no real secondary spikes from the previous summer spike.
The second chart below is the one I have been maintaining that is more of a curiosity to me than anything. However, it has been interesting to note that at the same time that the AZ DHS bed usage chart started to slow, the percent of 65+ year olds that was hospitalized one week after being diagnosed with COVID started to trend down too. If you scroll a bit on this site you’ll see that for a long time, the 65+ year old trend line (maroon) sloped upward while all other groups sloped downwards. Now they all slope downward, indicating that less people are being hospitalized after being diagnosed with COVID.
Below is another sign that the potency of the disease in society (note that the words “in society” are important here) is slowing. The below chart represents a comparison of deaths in people over 65 due to COVID with those in everyone else in the state. The green line is the 5 day moving average of the ratio of over65 to under65. Note that during the summer outbreak the ratio was pretty constant at around 2.5 deaths over 65 to 1 death under 65. During the virus’ “off-season” between August and November the ratio was all over the place because there were very few deaths. However, once the winter surge started, the ratio has been steadily increasing and hasn’t really gone down to the ratio of the summer months. What might this mean?
Perhaps the most susceptible people under 65 already died during the summer outbreak (or maybe they’re laying really low right now)? It does appear that people under 65 are far, far less susceptible to COVID absent comorbidities.
The overall death numbers in the over65 population do appear to the eye to be around the same as during the summer (but from my zip code analysis, they seem to be distributed more widely across the state). I wonder if this implies that there is a fixed number of people whose immune systems are “rigged” to fail under attack by COVID? Rigged, of course, through the mysterious operation of some unknown genetic markers or existing conditions of the immune system?
Finally, here’s a view of the case rates in both Pima (Red) and Maricopa (Blue) counties compared to the overall testing per day in the state (yellow). Note that testing peaked around Thanksgiving (probably people hoping to get a negative test prior to a Thanksgiving gathering). Testing seems to have fallen from Thanksgiving until New Years. Note that as the first wave flattened off around the start of August, testing decreased steadily. Since testing is an indicator of people that think they’re sick or think there may be a reason they’ve been exposed, it may well be that this is a sign of the surge slowing.