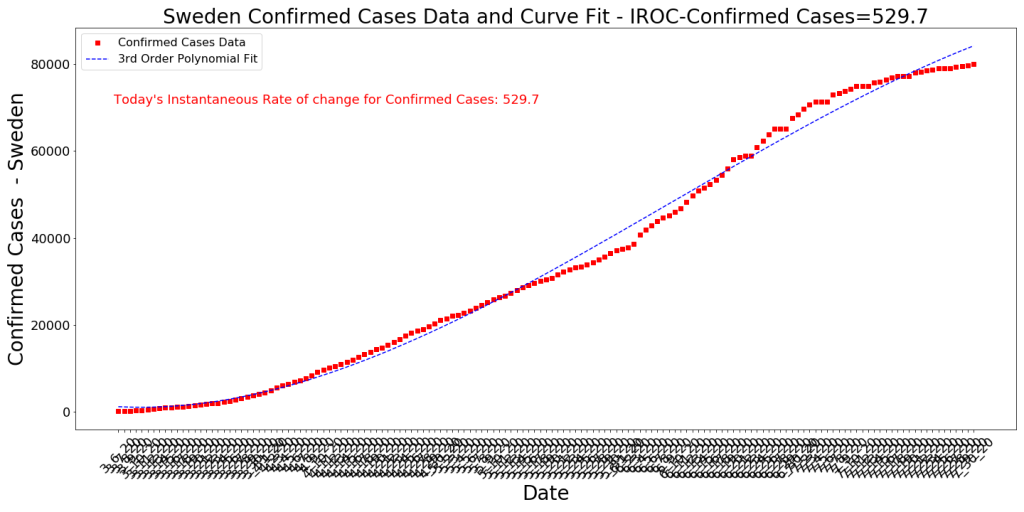
Arizona has seen its case growth numbers head towards zero for the last few weeks, but there may still be some value in exploring how the infection is affecting the state. Remember, tracking COVID cases is not useful in itself. Cases are a strong leading indicator, of course, of things we structurally care about as a state, such as hospital overtaxing and ultimately deaths. I believe this is the most productive mindset to have when approaching cases. Here is what the state’s cumulative Case curve looks like now.

We note that the Instantaneous Rate of Change (IROC) of the curve has now dropped to somewhere around 790. The trend is decreasing, however, as you can note about 4 days in a row where the rate appears to be approaching zero. We have three to four days of anomalous data from about 9/2 to 9/4, where the state appears to have been capturing University Antigen tests as confirmed cases. As the U of Arizona learned, at least, many of these Antigen positive results have turned out to be false positives when checked with a subsequent, more accurate PCR test. It appears from the data that 60-70 percent of the Antigen positive results are false positive. Since this realization, the state appears to only be counting the university cases if they’re confirmed with a PCR test. But not doing this for 3 days or so appears to have inflated our case numbers. Enough on that.
Zip Code Case Growth Update

This map doesn’t look much different than the previous week’s case increase map, except that there appears to be a bit higher numbers in Flagstaff (home of Northern Arizona University) and Prescott (home of Embry-Riddle University). But by far, the top two zip codes in case growth over the last week continue to be the homes of the University of Arizona and Arizona State. This is true even though the numbers of cases reported have dropped a bit due to only recording the cases confirmed with PCR.
Table of Zip Codes

The main thing to note here is that the top two are Tempe’s and Tucson’s University zip codes. Snowflake’s showing up as number three is a bit deceptive. They had 11 new cases this week, but they’ve only had 128 cases to date before this week. The 11 might be from one significant spreading event, or it could just be random noise. The 85009 zip code in Southwest Phoenix has been one that has had a handful of case spikes since Memorial day. The 200-ish new cases in that Zip code could be significant, especially since the Mexico-related infections from a month or two ago seem to have slowed significantly.
Conclusion
Data indicates that COVID-19 might be in the process of burning itself out in Arizona. For now at least… It will be interesting to see if the University cases lead to increased hospitalization numbers in their demographic about a week from now (so far, there hasn’t been any change). With this Zip Code approach above, we can also track if the University cases are spreading to adjacent or other Zip Codes.